
 Read on Twitter
Read on Twitter
*** COVID19 and males***
Is infection with SARS-CoV-2 more virulent among males, and if so why? Can we do anything about it, or use this information for treatment purposes. This thread is a compilation of thoughts & ideas by various colleagues: @AlanBryce9 & @lbaughn
#COVID19
1/x
Is infection with SARS-CoV-2 more virulent among males, and if so why? Can we do anything about it, or use this information for treatment purposes. This thread is a compilation of thoughts & ideas by various colleagues: @AlanBryce9 & @lbaughn
#COVID19
1/x
This thread is not meant to be comprehensive or curated. Furthermore, it is the work of others and we are only putting the ideas here to expand the conversation and stimulate further discussion. Add your thoughts, rebuttal or annotation.
https://www.nytimes.com/2020/02/20/health/coronavirus-men-women.html
https://www.nytimes.com/2020/02/2... href="https://twtext.com//hashtag/COVID19"> #COVID19
2/x
https://www.nytimes.com/2020/02/20/health/coronavirus-men-women.html
2/x
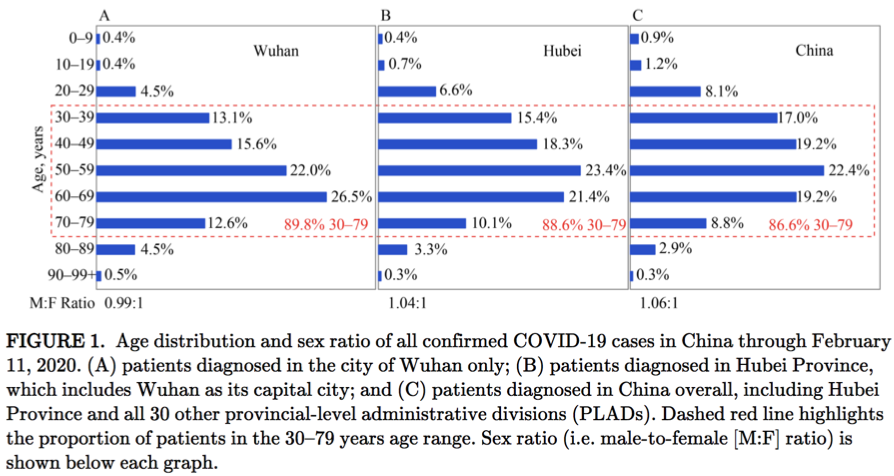
Infection risk and male mortality: The first reports from the CDC China shown no significant difference in the likelihood offing infected for males versus females
http://weekly.chinacdc.cn/en/article/id/e53946e2-c6c4-41e9-9a9b-fea8db1a8f51
https://weekly.chinacdc.cn/en/articl... href="https://twtext.com//hashtag/COVID19"> #COVID19
3/x
http://weekly.chinacdc.cn/en/article/id/e53946e2-c6c4-41e9-9a9b-fea8db1a8f51
3/x
 #COVID193/x" title="Infection risk and male mortality: The first reports from the CDC China shown no significant difference in the likelihood offing infected for males versus females https://weekly.chinacdc.cn/en/articl... href="https://twtext.com//hashtag/COVID19"> #COVID193/x" class="img-responsive" style="max-width:100%;"/>
#COVID193/x" title="Infection risk and male mortality: The first reports from the CDC China shown no significant difference in the likelihood offing infected for males versus females https://weekly.chinacdc.cn/en/articl... href="https://twtext.com//hashtag/COVID19"> #COVID193/x" class="img-responsive" style="max-width:100%;"/>
However, the case fatality rate was higher in males versus females for all patients (2.8% vs 1.7%). Age is a major prognostic factor, with much higher mortality observed among older individuals.
#COVID19
4/x
. Age is a major prognostic factor, with much higher mortality observed among older individuals. #COVID194/x")
#COVID19
4/x
This is confounded by lifestyle (smoking & obesity) plus co-morbidities (more common in males). A meta-analysis of 416 Chinese patients did not demonstrate sex to be a strong predictor. Also in China men smoke more.
https://jamanetwork.com/journals/jamacardiology/fullarticle/2763524
https://jamanetwork.com/journals/... href=" https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6546632/
https://www.ncbi.nlm.nih.gov/pmc/artic... href="https://twtext.com//hashtag/COVID19"> #COVID19
5/x
 plus co-morbidities (more common in males). A meta-analysis of 416 Chinese patients did not demonstrate sex to be a strong predictor. Also in China men smoke more. https://jamanetwork.com/journals/... href=")
https://jamanetwork.com/journals/jamacardiology/fullarticle/2763524
5/x
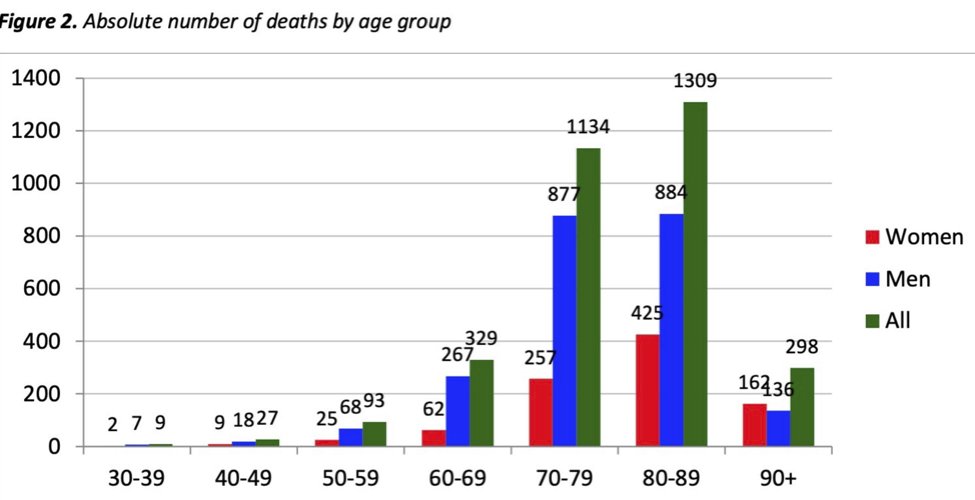
Also, a recent report from Italy shows higher mortality for males versus females. Among those deaths recorded over the age of 60 (n=3070), 2164 were males (70%)
HT @Mohty_EBMT
https://www.epicentro.iss.it/coronavirus/bollettino/Report-COVID-2019_20_marzo_eng.pdf
https://www.epicentro.iss.it/coronavir... href="https://twtext.com//hashtag/COVID19"> #COVID19
6/x
HT @Mohty_EBMT
https://www.epicentro.iss.it/coronavirus/bollettino/Report-COVID-2019_20_marzo_eng.pdf
6/x
 #COVID196/x" title="Also, a recent report from Italy shows higher mortality for males versus females. Among those deaths recorded over the age of 60 (n=3070), 2164 were males (70%)HT @Mohty_EBMT https://www.epicentro.iss.it/coronavir... href="https://twtext.com//hashtag/COVID19"> #COVID196/x" class="img-responsive" style="max-width:100%;"/>
#COVID196/x" title="Also, a recent report from Italy shows higher mortality for males versus females. Among those deaths recorded over the age of 60 (n=3070), 2164 were males (70%)HT @Mohty_EBMT https://www.epicentro.iss.it/coronavir... href="https://twtext.com//hashtag/COVID19"> #COVID196/x" class="img-responsive" style="max-width:100%;"/>
We find intriguing the link between androgens (receptor) & lung expression of the protein TMPRSS2, one of the coreceptors (with ACE2), and associated with SARS2 infectivity, shedding, & resistance to protective antibodies. TMPRSS is under androgenic control!
#COVID19
7/x
#COVID19
7/x
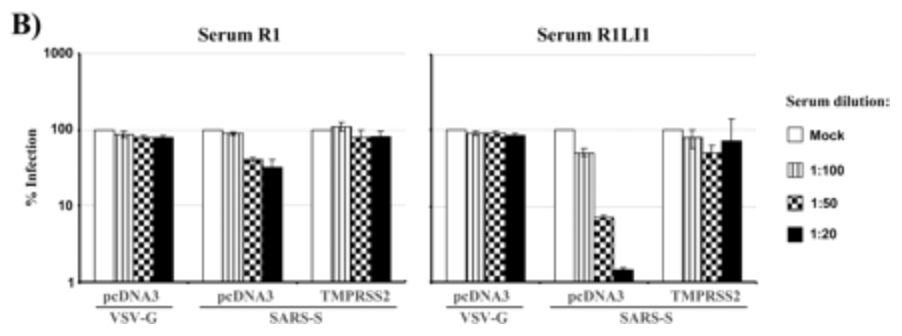
Previous work by Glowacka showed that the SARS S (spike) protein is proteolytically processed by TMPRSS2, and cleaved into several fragments upon coexpression of TMPRSS2 (cis-cleavage and trans-cleavage).
https://jvi.asm.org/content/85/9/4122
https://jvi.asm.org/content/8... href="https://twtext.com//hashtag/COVID19"> #COVID19
8/x
https://jvi.asm.org/content/85/9/4122
8/x
Cleavage resulted in the release of SARS S fragments to the cellular supernatant, inhibiting antibody-mediated neutralization. The graph shows viability in absence of TMPRSS2 (right) and reduced activity of protective antibodies (left)
https://jvi.asm.org/content/85/9/4122
https://jvi.asm.org/content/8... href="https://twtext.com//hashtag/COVID19"> #COVID19
9/x
https://jvi.asm.org/content/85/9/4122
9/x
 #COVID199/x" title="Cleavage resulted in the release of SARS S fragments to the cellular supernatant, inhibiting antibody-mediated neutralization. The graph shows viability in absence of TMPRSS2 (right) and reduced activity of protective antibodies (left) https://jvi.asm.org/content/8... href="https://twtext.com//hashtag/COVID19"> #COVID199/x" class="img-responsive" style="max-width:100%;"/>
#COVID199/x" title="Cleavage resulted in the release of SARS S fragments to the cellular supernatant, inhibiting antibody-mediated neutralization. The graph shows viability in absence of TMPRSS2 (right) and reduced activity of protective antibodies (left) https://jvi.asm.org/content/8... href="https://twtext.com//hashtag/COVID19"> #COVID199/x" class="img-responsive" style="max-width:100%;"/>
TMPRSS2 protein & ACE2 protein are overlapping. Lung epithelium was analyzed by immunohistochemistry- TMPRSS2 and ACE2 demonstrated strong positive staining of type II pneumocytes (P2) and alveolar macrophages (M), while type I pneumocytes were negative (P1)
#COVID19
10/x
 and alveolar macrophages (M), while type I pneumocytes were negative (P1) #COVID1910/x")
#COVID19
10/x
Overall expression across different tissues of TMPRSS2 is highest in prostate. It is also high in stomach, intestine, colon (could this explain some of the GI issues), and lung you see in green.
https://www.proteinatlas.org/ENSG00000184012-TMPRSS2/tissuecid:image001.jpg@01D60732.89F96330">https://www.proteinatlas.org/ENSG00000...
, and lung you see in green. https://www.proteinatlas.org/ENSG00000...")
https://www.proteinatlas.org/ENSG00000184012-TMPRSS2/tissuecid:image001.jpg@01D60732.89F96330">https://www.proteinatlas.org/ENSG00000...
Previous work studying other coronaviruses shows TMPRSS2 contributes to virus spread & pathology in murine models. TMPRSS2 activates the spike protein of highly pathogenic human coronaviruses (& influenza too).
https://doi.org/10.1128/JVI.01815-18
https://doi.org/10.1128/J... href="https://twtext.com//hashtag/COVID19"> #COVID19
11/x
https://doi.org/10.1128/JVI.01815-18
11/x
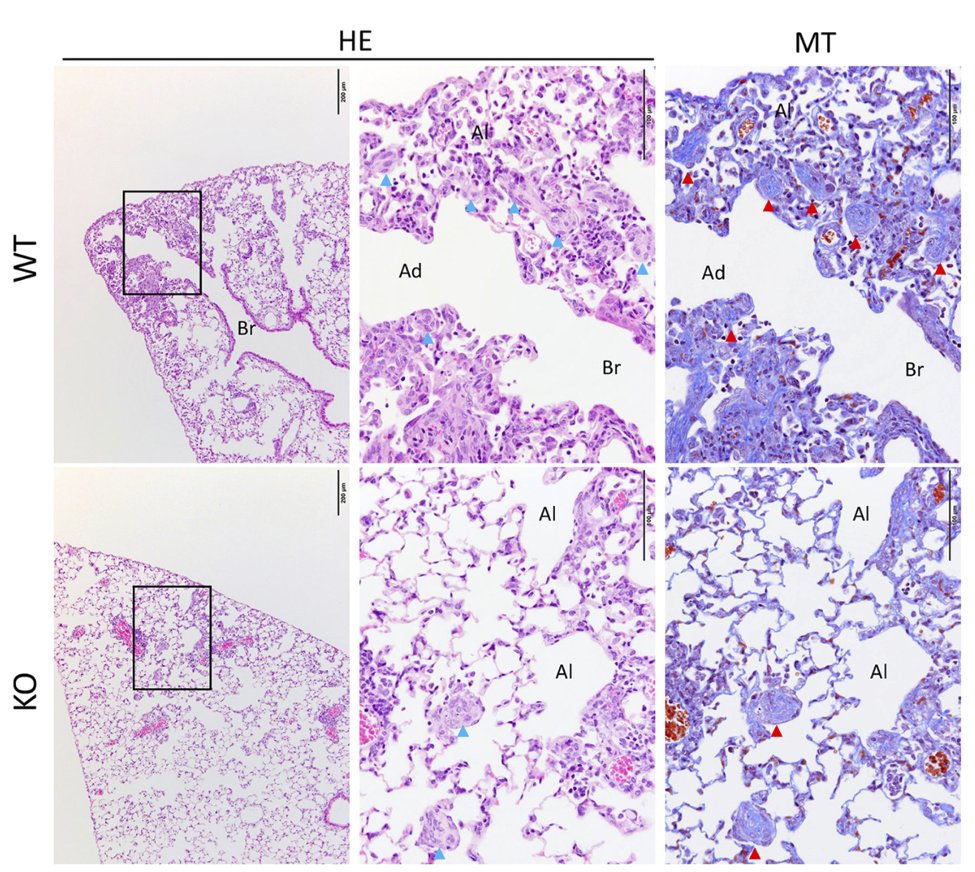
Using TMPRSS2-knock out (KO) mice the investigators showed a weakened inflammatory chemokine and/or cytokine response. Lung inflammatory reactions were less pronounced in the KO mice. Granulation tissue (Masson bodies, shown by arrows)
https://doi.org/10.1128/JVI.01815-18
https://doi.org/10.1128/J... href="https://twtext.com//hashtag/COVID19"> #COVID19
12/x
https://doi.org/10.1128/JVI.01815-18
12/x
 #COVID1912/x" title="Using TMPRSS2-knock out (KO) mice the investigators showed a weakened inflammatory chemokine and/or cytokine response. Lung inflammatory reactions were less pronounced in the KO mice. Granulation tissue (Masson bodies, shown by arrows) https://doi.org/10.1128/J... href="https://twtext.com//hashtag/COVID19"> #COVID1912/x" class="img-responsive" style="max-width:100%;"/>
#COVID1912/x" title="Using TMPRSS2-knock out (KO) mice the investigators showed a weakened inflammatory chemokine and/or cytokine response. Lung inflammatory reactions were less pronounced in the KO mice. Granulation tissue (Masson bodies, shown by arrows) https://doi.org/10.1128/J... href="https://twtext.com//hashtag/COVID19"> #COVID1912/x" class="img-responsive" style="max-width:100%;"/>
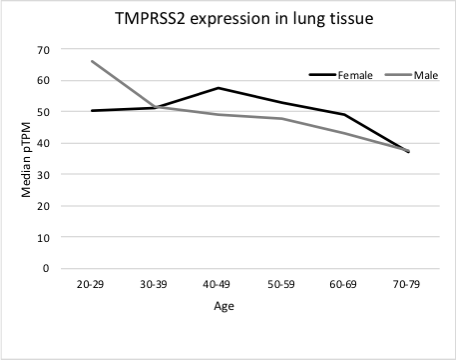
We were interested to see if age/sex determines TMPRSS2 lung protein. Based on the Protein Atlas data, only males in the 20-29 year age group express more TMPRSS2 in the lung compared to females- we cannot rule out a functional link.
https://www.proteinatlas.org/ENSG00000184012-TMPRSS2/tissue/lung
https://www.proteinatlas.org/ENSG00000... href="https://twtext.com//hashtag/COVID19"> #COVID19
13/x
https://www.proteinatlas.org/ENSG00000184012-TMPRSS2/tissue/lung
13/x
 #COVID1913/x" title="We were interested to see if age/sex determines TMPRSS2 lung protein. Based on the Protein Atlas data, only males in the 20-29 year age group express more TMPRSS2 in the lung compared to females- we cannot rule out a functional link. https://www.proteinatlas.org/ENSG00000... href="https://twtext.com//hashtag/COVID19"> #COVID1913/x" class="img-responsive" style="max-width:100%;"/>
#COVID1913/x" title="We were interested to see if age/sex determines TMPRSS2 lung protein. Based on the Protein Atlas data, only males in the 20-29 year age group express more TMPRSS2 in the lung compared to females- we cannot rule out a functional link. https://www.proteinatlas.org/ENSG00000... href="https://twtext.com//hashtag/COVID19"> #COVID1913/x" class="img-responsive" style="max-width:100%;"/>
TM-RSS2 could have yet to be defined interactions in the androgen receptor signaling that may play a role in added virulence in males. A hypothesis only of course. Others know better!
https://pathcards.genecards.org/card/coregulation_of_androgen_receptor_activity
https://pathcards.genecards.org/card/core... href=" https://string-db.org/network/9606.ENSP00000381588
https://string-db.org/network/9... href="https://twtext.com//hashtag/COVID19"> #COVID19
14/x

https://pathcards.genecards.org/card/coregulation_of_androgen_receptor_activity
14/x
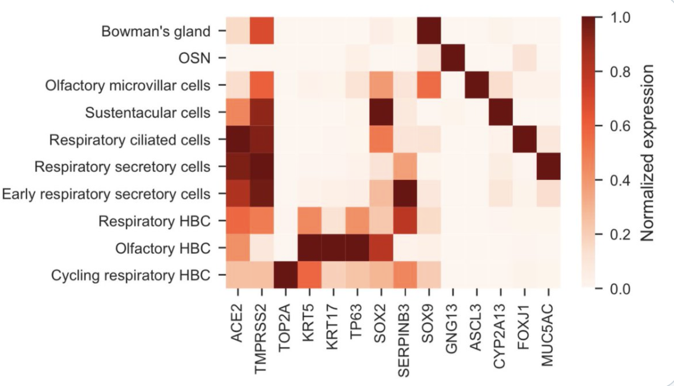
The interaction between the virus and the receptor may manifest itself clinically elsewhere. For instance, there is good data that relates it to anosmia, as reported by many patients, and as shown by the expression graph below.
HT @StearnsLab
https://www.biorxiv.org/content/10.1101/2020.03.25.009084v1
https://www.biorxiv.org/content/1... href="https://twtext.com//hashtag/COVID19"> #COVID19
15/x
HT @StearnsLab
https://www.biorxiv.org/content/10.1101/2020.03.25.009084v1
15/x
 #COVID1915/x" title="The interaction between the virus and the receptor may manifest itself clinically elsewhere. For instance, there is good data that relates it to anosmia, as reported by many patients, and as shown by the expression graph below.HT @StearnsLab https://www.biorxiv.org/content/1... href="https://twtext.com//hashtag/COVID19"> #COVID1915/x" class="img-responsive" style="max-width:100%;"/>
#COVID1915/x" title="The interaction between the virus and the receptor may manifest itself clinically elsewhere. For instance, there is good data that relates it to anosmia, as reported by many patients, and as shown by the expression graph below.HT @StearnsLab https://www.biorxiv.org/content/1... href="https://twtext.com//hashtag/COVID19"> #COVID1915/x" class="img-responsive" style="max-width:100%;"/>
One clinical trial is testing an inhibitor of TMPRSS2, camostat mesylate (CM) at the University of Aarhus ( http://ClinicalTrials.gov"> http://ClinicalTrials.gov Identifier: NCT04321096) It is a Phase 1/2 Clinical trial (2x100 mg pills 3 times daily for 5 days) PI Ole S Søgaard, MD PhD
#COVID19
16/x
 at the University of Aarhus ( http://ClinicalTrials.gov Identifier: NCT04321096) It is a Phase 1/2 Clinical trial (2x100 mg pills 3 times daily for 5 days) PI Ole S Søgaard, MD PhD #COVID1916/x")
#COVID19
16/x
CM has been mentioned by others. It is an approved drug in Japan for the treatment of pancreatic inflammation and esophagitis.
HT via @PeterKolchinsky
https://twitter.com/PeterKolchinsky/status/1240411694855266304?s=20
https://twitter.com/PeterKolc... href="https://twtext.com//hashtag/COVID19"> #COVID19
17/x
HT via @PeterKolchinsky
https://twitter.com/PeterKolchinsky/status/1240411694855266304?s=20
17/x
 #COVID1917/x" title="CM has been mentioned by others. It is an approved drug in Japan for the treatment of pancreatic inflammation and esophagitis.HT via @PeterKolchinsky https://twitter.com/PeterKolc... href="https://twtext.com//hashtag/COVID19"> #COVID1917/x" class="img-responsive" style="max-width:100%;"/>
#COVID1917/x" title="CM has been mentioned by others. It is an approved drug in Japan for the treatment of pancreatic inflammation and esophagitis.HT via @PeterKolchinsky https://twitter.com/PeterKolc... href="https://twtext.com//hashtag/COVID19"> #COVID1917/x" class="img-responsive" style="max-width:100%;"/>
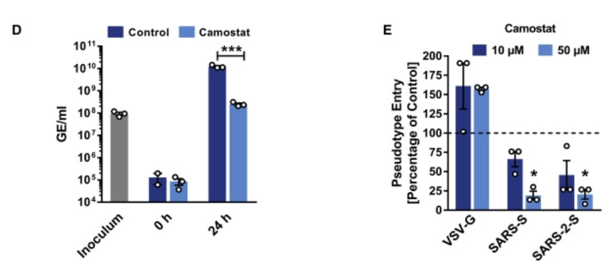
A recent Cell paper shows the efficacy of CM in vitro models. This study provides evidence that host cell entry of SARS-CoV-2 depends on TMPRSS2 & ACE2, and can be blocked by an inhibitor of the cellular serine protease TMPRSS2 CM.
https://www.cell.com/cell/fulltext/S0092-8674(20)30229-4?rss=yes#%20
https://www.cell.com/cell/full... href="https://twtext.com//hashtag/COVID19"> #COVID19
18/x
https://www.cell.com/cell/fulltext/S0092-8674(20)30229-4?rss=yes#%20
18/x
 #COVID1918/x" title="A recent Cell paper shows the efficacy of CM in vitro models. This study provides evidence that host cell entry of SARS-CoV-2 depends on TMPRSS2 & ACE2, and can be blocked by an inhibitor of the cellular serine protease TMPRSS2 CM. https://www.cell.com/cell/full... href="https://twtext.com//hashtag/COVID19"> #COVID1918/x" class="img-responsive" style="max-width:100%;"/>
#COVID1918/x" title="A recent Cell paper shows the efficacy of CM in vitro models. This study provides evidence that host cell entry of SARS-CoV-2 depends on TMPRSS2 & ACE2, and can be blocked by an inhibitor of the cellular serine protease TMPRSS2 CM. https://www.cell.com/cell/full... href="https://twtext.com//hashtag/COVID19"> #COVID1918/x" class="img-responsive" style="max-width:100%;"/>
Calu-3 cells were pre-incubated with CM and infected with SARS-CoV-2 (D). Genome equivalents in culture supernatants were determined by qRT-PCR. They also investigate whether TMPRSS2 is required for SARS-2-S-driven entry to lung cells (E).
https://www.cell.com/cell/fulltext/S0092-8674(20)30229-4?rss=yes#%20
https://www.cell.com/cell/full... href="https://twtext.com//hashtag/COVID19"> #COVID19
19/x
https://www.cell.com/cell/fulltext/S0092-8674(20)30229-4?rss=yes#%20
19/x
 #COVID1919/x" title="Calu-3 cells were pre-incubated with CM and infected with SARS-CoV-2 (D). Genome equivalents in culture supernatants were determined by qRT-PCR. They also investigate whether TMPRSS2 is required for SARS-2-S-driven entry to lung cells (E). https://www.cell.com/cell/full... href="https://twtext.com//hashtag/COVID19"> #COVID1919/x" class="img-responsive" style="max-width:100%;"/>
#COVID1919/x" title="Calu-3 cells were pre-incubated with CM and infected with SARS-CoV-2 (D). Genome equivalents in culture supernatants were determined by qRT-PCR. They also investigate whether TMPRSS2 is required for SARS-2-S-driven entry to lung cells (E). https://www.cell.com/cell/full... href="https://twtext.com//hashtag/COVID19"> #COVID1919/x" class="img-responsive" style="max-width:100%;"/>
None of the strategies targeting the receptor would show up in a broad search for antiviral compounds since they will likely look mostly at the direct antiviral activity of the various compounds. Several elegant studies are underway.
https://biorxiv.org/content/10.1101/2020.03.25.008482v1?rss=1
HT">https://biorxiv.org/content/1... @DrChoueiri
21/x

https://biorxiv.org/content/10.1101/2020.03.25.008482v1?rss=1
HT">https://biorxiv.org/content/1... @DrChoueiri
21/x
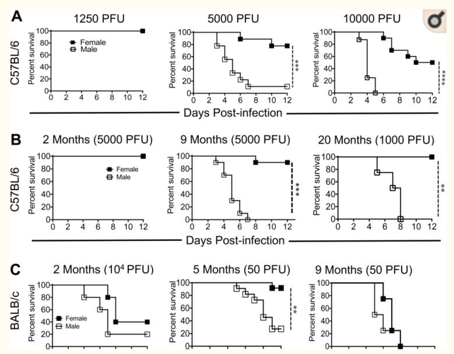
Many questions remain. During the MERS epidemic the mortality was also higher for men. In one murine study for SARS male mice fared worse than females. However, in this study ovaries appeared to be protective.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5450662/
https://www.ncbi.nlm.nih.gov/pmc/artic... href="https://twtext.com//hashtag/COVID19"> #COVID19
22/x
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5450662/
22/x
 #COVID1922/x" title="Many questions remain. During the MERS epidemic the mortality was also higher for men. In one murine study for SARS male mice fared worse than females. However, in this study ovaries appeared to be protective. https://www.ncbi.nlm.nih.gov/pmc/artic... href="https://twtext.com//hashtag/COVID19"> #COVID1922/x" class="img-responsive" style="max-width:100%;"/>
#COVID1922/x" title="Many questions remain. During the MERS epidemic the mortality was also higher for men. In one murine study for SARS male mice fared worse than females. However, in this study ovaries appeared to be protective. https://www.ncbi.nlm.nih.gov/pmc/artic... href="https://twtext.com//hashtag/COVID19"> #COVID1922/x" class="img-responsive" style="max-width:100%;"/>
We are also intrigued by the possibility that polymorphisms in the androgen and androgen receptor pathway may dictate virulence in different populations, and indirectly via TMPRSS2. One GWAS study found 71 loci associated with susceptibility.
https://www.nature.com/articles/s41467-017-01490-8
23/x">https://www.nature.com/articles/...
https://www.nature.com/articles/s41467-017-01490-8
23/x">https://www.nature.com/articles/...
It is impossible to find a reliable map of the male baldness pater distribution. The three found are shown here (some disputed). Interestingly, the distribution in the three of them seem to show coincidence with areas of high virulence. Big grain of salt though!
#COVID19
24/x
. Interestingly, the distribution in the three of them seem to show coincidence with areas of high virulence. Big grain of salt though! #COVID1924/x")
. Interestingly, the distribution in the three of them seem to show coincidence with areas of high virulence. Big grain of salt though! #COVID1924/x")
. Interestingly, the distribution in the three of them seem to show coincidence with areas of high virulence. Big grain of salt though! #COVID1924/x")
#COVID19
24/x
Conclusion: It is possible but unproven that males fare worse due to the link between the androgen receptor & TMPRSS2- we cannot rule out a functional effect via AR. CM should be tested as a treatment against COVID-19, perhaps alone or in combination with androgen blockade.
End
End


